
A look at how Virginia may work to decrease ED overutilization
VACEP weighs in on new report from
state health care Commission
For emergency physicians, it’s not news to learn EDs are full of patients who have nowhere else to turn.
But, at long last, the Virginia government finally delved in deeper to look at why so many patients are sicker and visiting the ED more often.
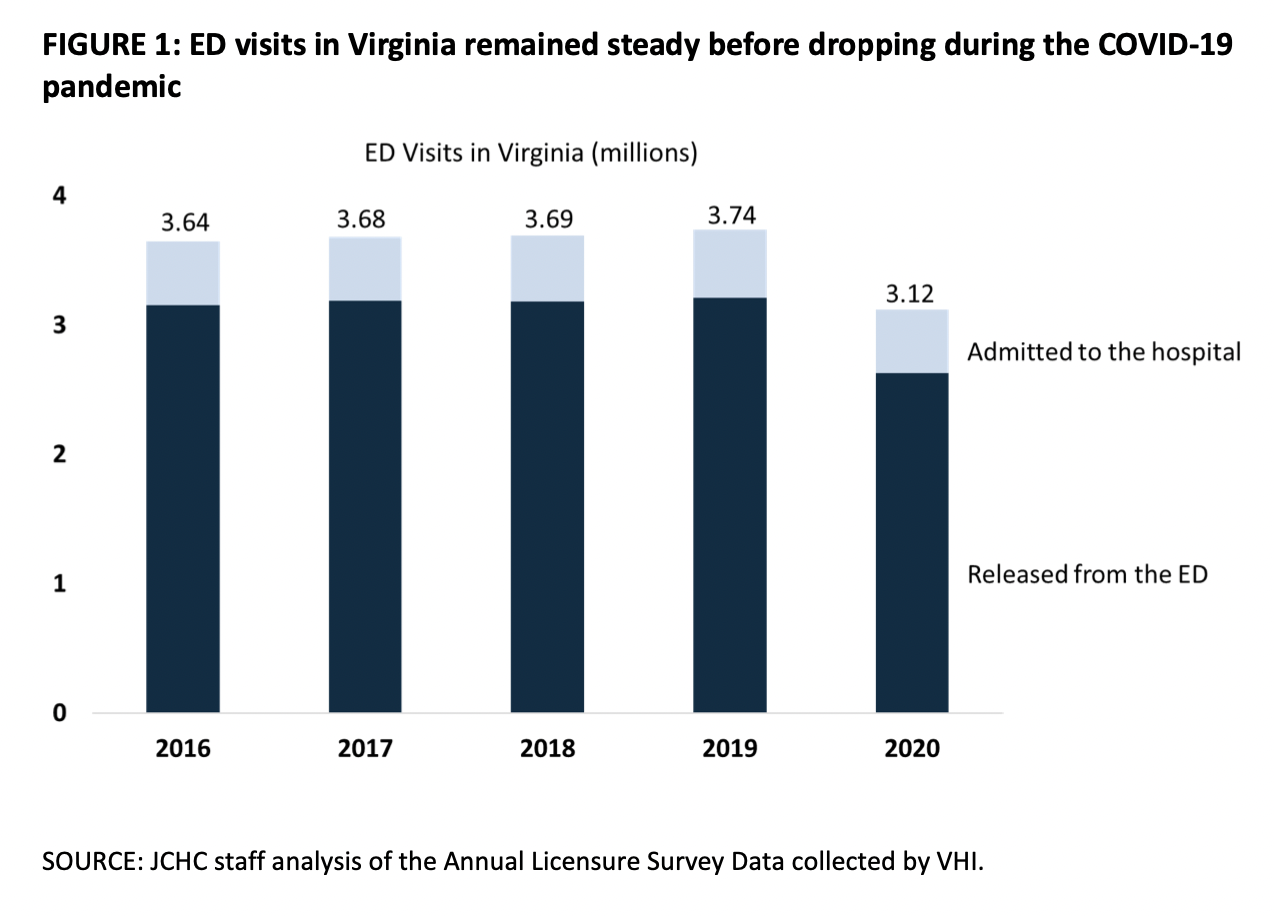
ED visits in Virginia remained steady from 2016-2019 before declining in 2020, reflecting the impact of the COVID-19 pandemic. An increasing number of visits for mental health and substance abuse issues were a contributing factor to these trends.
This month, the legislative branch’s Joint Commission on Health Care released a report, Reducing Unnecessary Emergency Department Utilization. It was sent to General Assembly members and Gov. Glenn Youngkin’s office, and includes six recommended options state leaders can pursue to ensure Virginians are treated in the most appropriate setting — including primary care, pediatrician offices, urgent care and other preventive locations — to reduce the burden on emergency departments.

Todd Parker, MD, FACEP
VACEP President
Commission staff reviewed types and severity of conditions commonly treated in EDs, assessed how health insurance coverage and primary care access impact utilization, and considered how free-standing EDs influence cost and access.
Staff also consulted the experts at VACEP, with a researcher visiting nearly two dozen ERs statewide — including Riverside Health System, where VACEP President Todd Parker, MD, FACEP practices.
“Many of the trends highlighted in the report are what we are seeing every day in our emergency departments,” wrote Parker in a September 30 letter to Jeffrey Lunardi, the Commission’s Executive Director.
Those trends: increasing acuity of patients; a higher than normal volume of behavioral health and substance abuse patients, with ever increasing wait times for in-patient psychiatric care; patients returning because they cannot get primary care appointments, often for months; and urgent care centers having to reduce their hours due to staffing.
In weighing options, Parker stressed the importance of EMTALA and prudent layperson, “the lens that we as physicians must look at someone presenting in the emergency department.”
“It is then incumbent upon us to appropriately medically screen [patients], determine their emergency, and stabilize them,” he wrote. “These are patient safety laws that were enacted to ensure fair and equal treatment of patients, regardless of their ability to pay and we strongly stand by these important guidelines.”
Overall, VACEP supported most of the Commission’s recommended options and opposed one. More importantly, VACEP asked the Commission to go further by making additional policy option requests.
In Support
Option 1: Direct DMAS to collect and report on claim denials from MCOs by provider type.
Per Parker: “Further identifying what those payment barriers may be and how they vary by specialty is important. We would ask that emergency physicians also be included when looking at MCO claim denials because we are the only physician specialty who takes care of all patients, including Medicaid.”
Option 2: Direct a study of primary care practice scheduling processes for Medicaid enrollees, including whether Medicaid enrollees are able to get appointments in compliance with MCO contract.
VACEP agreed, and pushed the Commission expand the study. “We ask that this policy option be broadened to include a deeper analysis of how we are truly defining and tracking Medicaid MCO network adequacy when it comes to patient access to primary care physicians,” Parker wrote. “Appointment availability in a timely manner needs to be addressed. A network should not be considered ‘adequate’ if Medicaid patients who come to the ER cannot then get a primary care appointment for six months or longer…without places to refer patients, they will have no choice but to return to the ED for care when their condition worsens.”

The intensity of services for patients increased during the pandemic, and the average cost of an ED visit increased by 41.5%.
Options 3 and 4: Establish two grant programs for hospital and ambulance-based care management.
Parker agreed: “It makes sense to look to EMS and first responders as continued allies in the effort to reduce ER utilization.”
Option 5: Require hospitals to submit Emergency Severity Index (ESI) codes, reason codes, and social determinant of health Z-codes on claims and require them to be submitted to the All-Payer Claims Database.
While generally supportive, “it’s important that all the coding participants agree that having these codes collected and submitted are useful and appropriate,” Parker wrote. “Having ‘clean claims’ is an issue on the payment side and we would not support having these codes collected and then the insurers rejecting the claims because having the codes on there are not technically diagnostic in nature. We do not support additional administrative burdens that do not benefit the patients we are caring for.”
In Opposition
Option 6: Require freestanding emergency departments to better identify themselves to patients.
Parker told the Commission that any further signage requirements beyond “Emergency Department” may discourage someone who is having an emergency from seeking care. “As emergency physicians, we do not support any barriers to patients seeking emergency care who need it right away,” Parker wrote. “Any regulations that make patients second guess seeking treatment, especially for potential financial reasons, is in direct opposition to the federal EMTALA law that governs patient care.”
He added that providing information through signage to a patient when they are in the ED or telling them about financial issues could violate EMTALA.
Though not included in report’s recommended options, VACEP pushed the Commission to repeal the Virginia budget policy of automatically downcoding fees for emergency department visits based solely on a diagnosis list of nearly 800 common, medium, and high-risk codes. (Get the latest on the Downcoding Provision here.)

Conditions such as diabetes, hypertension, and asthma can be treated and managed, but often result in ED visits if patients don’t get the care they need. Additionally, the vast majority of high utilizers of the ED have mental health or substance abuse diagnoses. Hospital-based and ambulance-based care management programs can be effective at better managing these conditions in the community, the report said.
“There is no evidence that this policy reduces ER utilization or changes patient behavior,” Parker wrote. “All it does is single out the one set of physicians who are mandated by EMTALA to evaluate and treat patients without regard of their ability to pay and penalizes the physicians for providing care to [Medicaid] patients.”
Additionally, VACEP asked the Commission to include recommendations from a Virginia Department of Medical Assistance Services (DMAS) workgroup from 2020 that developed its own set of recommendations to reduce ED utilization and improve care coordination. That report recommended:
Increasing primary care rates to promote increased access to care
Including coverage of, and payment for, complex chronic care management services
Targeting increased payment rates for access-promoting services
Developing embedded care coordination models in areas with high behavioral health needs
Increasing access to behavioral health providers in the continuum
Funding direct connection between MCOs and a community-based organization network coordinate to address related social needs
Finally, Parker asked the Commission to investigate Medicaid MCO compliance with existing contract provisions related to reducing non-emergent and preventable ED visits and coordination of care and related performance metrics. He told the Commission to investigate the effectiveness of these provisions and related performance and outcomes “to determine if Medicaid MCOs are following their contractual obligations to DMAS and Medicaid enrollees and whether any modifications are required.”
But overall, Parker noted: “As an emergency physician, I can safely say this is the first time someone from the state looking into patient utilization of the emergency department came and spoke to us in our workplace and I cannot over emphasize how impactful that was to us and I hope, to him.”
