

Management of Blunt Cerebrovascular Injury
By Joshua Easter, MD, MSc
University of Virginia Health System emergency physician and UVA School of Medicine associate professor
Case: A 70-year-old female with a history of hypertension presents to your ED after a fall down 3 steps. She is not anticoagulated, has normal vital signs, and a normal level of alertness. She has a small hematoma over her occiput and pain over her superior cervical spine. CT of her head and cervical spine reveals a basilar skull fracture. In addition to consultation with a neurosurgeon, how else will you evaluate and manage her trauma?
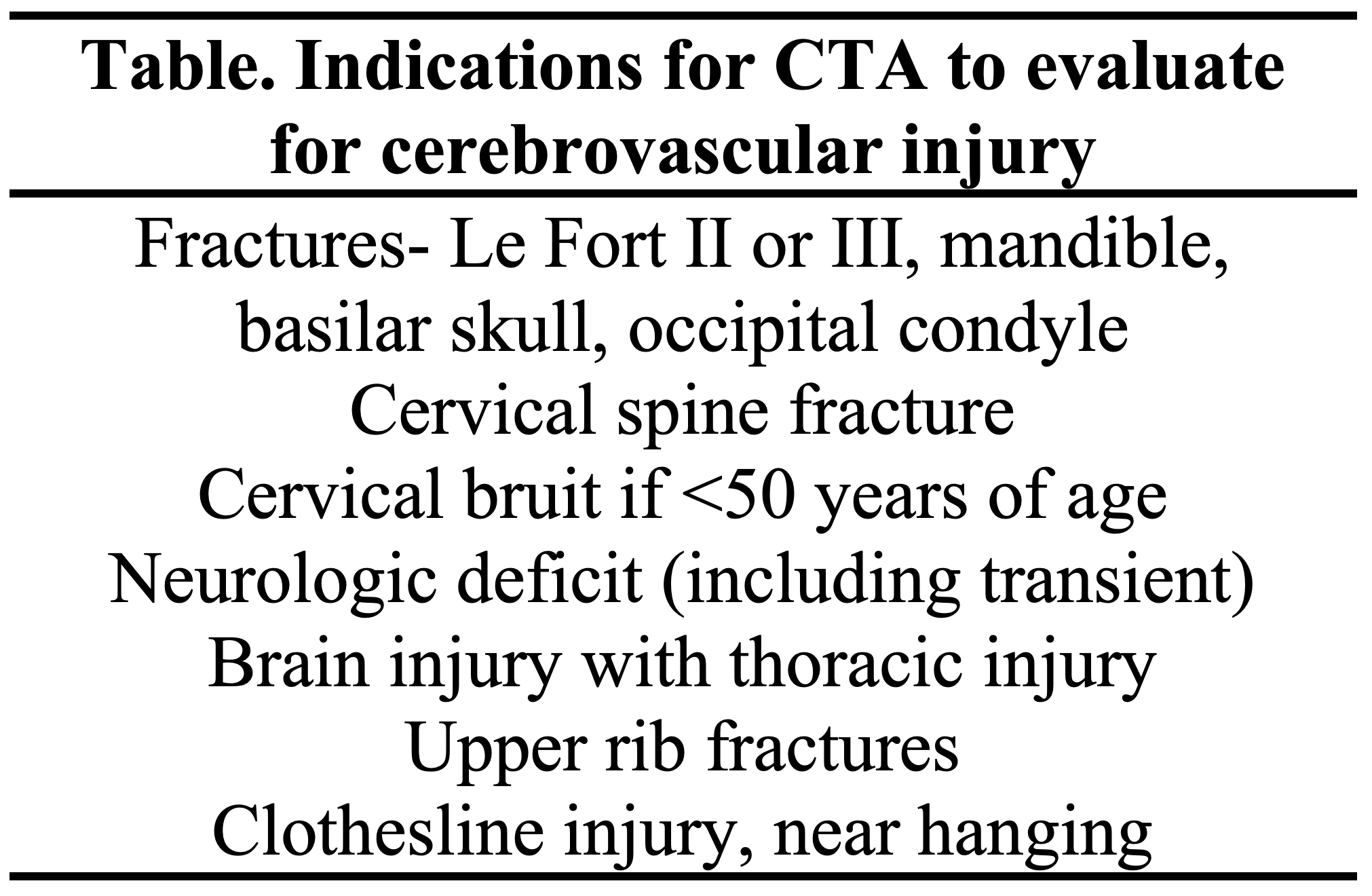
Blunt traumatic injuries to the carotid and vertebral arteries are rare, occurring in 1-3% of admitted trauma patients (Miller, 2002). They most commonly arise after motor vehicle collisions or falls in the elderly. Initially patients tend to be asymptomatic but as thrombi form and impede flow or embolize to the cerebral circulation, patients may develop signs of stroke, including neurologic deficits (Biffl, 2002). These injuries can be life threatening, leading to death in approximately one in four patients (Biffl, 1998). Blunt cerebrovascular injuries are most common in patients with severe mechanisms of injury, and patients often harbor other injuries, particularly cervical spine (OR=.5.5) or chest trauma (OR=2.0) (Franz, 2012). Certain injuries should typically prompt evaluation for cerebrovascular injury with CT angiography (CTA) (Table).
Once identified the appropriate management of blunt cerebrovascular injuries is unclear. Antithrombotic agents, including antiplatelet and anticoagulants, appear to reduce the risk of stroke in single center studies (Emmett, 2011; Biffl, 2002; Cothren, 2009). However, there is concern these agents may increase the severity of hemorrhage in trauma patients and worsen outcomes (e.g., patient with intracranial hemorrhage and carotid dissection). As a result, 25-40% of patients with known blunt cerebrovascular injuries are not treated with antithrombotics (Burlew, 2018). The exact risks associated with not treating blunt cerebrovascular injuries are unknown, and this study aimed to quantify this risk.
Russo et al. completed a retrospective review of all blunt cerebrovascular injuries in the American Association for the Surgery of Trauma’s multicenter Prospective Vascular Injury Treatment (PROOVIT) registry from 2013-19 (Russo, 2021). Patients >2 years of age with injuries to their cerebrovascular vessels were prospectively enrolled in the database. Patients were considered to have received antithrombotics, if they were treated at any point during their hospitalization with antiplatelet agents (e.g., aspirin, clopidogrel) or anticoagulants (e.g., heparin, low molecular weight heparin, warfarin, or rivaroxaban). Patients receiving DVT prophylaxis with anticoagulants were not considered to have received treatment. The primary outcomes were stroke or death after >24 hours, as the authors believed earlier deaths were unlikely to have arisen as a result of the cerebrovascular injury or treatment with antithrombotics. The authors performed multivariate regression analysis, utilizing a clustered regression trees approach to account for differences by facility. They stratified results by the grade of the injury from I-V (I/II had flow limiting dissections, III had pseudoaneurysms, IV had occlusions, and V had transections of the artery).
They identified 920 patients with 971 blunt cerebrovascular injuries. Nearly two thirds (62%) were low grade (I or II) flow limiting dissections, and <2% were grade V transections. Almost all injuries (92%) were diagnosed by CT angiography. One in five patients did not receive antithrombotic therapy at any point during their hospitalization, and they had higher injury severity scores and lower Glasgow Coma Scale scores compared to patients that received antithrombotic therapy. Overall, 7% of patients experienced a stroke, and these patients were more likely to die (OR=4.2, 95% CI, 1.4-12). Patients with higher grade injuries were more likely to suffer strokes and die.
Treatment with antithrombotics was associated with reduced risk of stroke (OR=0.35; 95% CI: 0.21-0.57), death (OR=0.09; 95% CI: 0.06-0.13) and a composite outcome of stroke or death (OR=0.08; 95% CI: 0.06-0.11). The significant beneficial effects of treatment on death and the composite outcome of stroke or death persisted in multivariate modeling controlling for co-variates, such as demographics and co-morbid injuries. Benefits of therapy were present in all grades of cerebrovascular injury, including low grade injuries. Although, the benefits of therapy tended to be greater for patients with higher grade cerebrovascular injuries Treatment with anticoagulants or antithrombotics showed similar positive effects. Combination therapy with both agents was not more beneficial than use of a single agent.
While this is the largest study to date to assess the benefits of treatment with antithrombotics, the primary limitation of this study is its retrospective nature. Due to this, the authors were unable to ascertain the potential adverse effects of antithrombotic therapy. While they did measure the most feared complication of death, they did not assess other complications, such as hemorrhage and need for operative intervention. A recent meta-analysis found 2-6% of trauma patients experienced hemorrhage after antithrombotic treatment; although, they did not quantify the severity of the hemorrhage (Ku, 2021). Antiplatelet agents harbored a lower risk of hemorrhage than anticoagulants (OR=0.38; 95% CI: 0.15-1.0) (Ku, 2021).
Emergency medicine physicians should have a high suspicion for blunt cerebrovascular injuries in patients with high mechanism trauma or injuries to the cervical spine, face, or chest. Patients should undergo CTA to detect these injuries. When cerebrovascular injuries are present it is appropriate to initiate antithrombotic therapy, and antiplatelet agents appear potentially safer than anticoagulants. If a concomitant injury is present that might increase the risks from hemorrhage, it would be prudent to discuss initiation of antithrombotic therapy with a trauma surgeon.
Your patient’s basilar skull fracture is a risk factor for blunt cerebrovascular injury (Table). Therefore, she should undergo CT angiography to evaluate her carotid and vertebral arteries. This reveals a small dissection with <25% stenosis of her carotid artery. The patient has no other injuries. After discussion with the neurosurgeon, you elect to administer aspirin to reduce the risk of stroke and death for you
About the VACEP EM Lit Review: Every month, VACEP members will share their readings of the latest medical literature. Submit yours to us by emailing Executive Director Sarah Marshall.
